
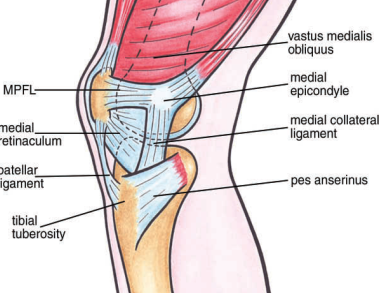
 Lateral patellar instability is almost always due to a patellar (kneecap) dislocation. In this circumstance, an athlete or patient will experience their kneecap slipping out of the lateral (outside) aspect of their knee. It almost always occurs with the knee straight or at shallow degrees of knee flexion rather than with the knee bent. When the patella dislocates, it tears the structures on the inside of the knee, with the medial patellofemoral ligament (MPFL) most commonly torn.
Lateral patellar instability is almost always due to a patellar (kneecap) dislocation. In this circumstance, an athlete or patient will experience their kneecap slipping out of the lateral (outside) aspect of their knee. It almost always occurs with the knee straight or at shallow degrees of knee flexion rather than with the knee bent. When the patella dislocates, it tears the structures on the inside of the knee, with the medial patellofemoral ligament (MPFL) most commonly torn.
Symptoms of lateral patellar instability:
• Feeling of kneecap slipping with twisting or turning movements
• In rare cases a near knee dislocation (subluxation) when the knee is close to being straight
TREATMENT FOR LATERAL PATELLAR INSTABILITY
There are many factors to evaluate in a patient’s prognosis when a lateral patellar dislocation exists. The cause of lateral patellar instability is very important to thoroughly evaluate, and each patient should be evaluated in terms of history, physical exam, X-rays, and MRI scans to determine the best treatment for them.
In the majority of circumstances, we treat these without surgery and attempt rehabilitation. Patients who have a normal patellar height and when injured, do not knock off any pieces of articular cartilage or bone, have a fairly good prognosis and have a low risk of recurrent patellar instability. However, in patients that are young and have dislocated their kneecaps previously, or in patients with conditions called patella alta, or trochlear dysplasia, there is a much higher risk of recurrent lateral patellar instability. However, in most of these patients, we still would recommend a formal non-operative rehabilitation program to assess their prognosis.
Patients who have recurrent instability may need surgery to restore both the medial stabilizing ligaments of the knee and any other associated pathology. This can include a medial patellofemoral ligament reconstruction, a lateral retinacular lengthening, a tibial tubercle osteotomy, and/or a trochleoplasty.
POST-OP
Patients who undergo a MPFL reconstruction must be non-weightbearing for 6 weeks after surgery. Knee motion is limited to 90 degrees for the first two weeks after surgery and then full motion is allowed. At six weeks after surgery, weight bearing is commenced and patients may wean off crutches when they can ambulate without a limp. The use of a stationary bike is also initiated at 6 weeks after surgery and endurance and agility exercises are initiated at 3 months after surgery. Most patients without any arthritis in their kneecap can return to full sporting activities at between 5-6 months after surgery.
See full story on drrobertlaprademd.com